Moana Medical Supply System | Moana Digital Health
The Moana Medical Supply System connects every facility, every province, and national procurement in one real-time supply chain platform, built for governments managing medicine availability across large, low-connectivity facility networks.
" height="11.607177083333333px" id="F3jyorGue" transform="translate(1.339 8.927)" width="22.321395833333213px"/><path d="M 0.874 3.575 L 10.021 9.486 C 10.367 9.71 10.764 9.821 11.161 9.821 C 11.558 9.821 11.954 9.71 12.301 9.486 L 21.447 3.575 C 21.995 3.221 22.321 2.63 22.321 1.991 C 22.321 0.893 21.4 0 20.267 0 L 2.054 0 C 0.921 0 0 0.893 0 1.992 C 0 2.63 0.327 3.221 0.874 3.575 Z" fill="rgb(27, 18, 61)" height="9.821395833333332px" id="KOAXH2cGk" transform="translate(1.339 4.464)" width="22.321395833333213px"/></svg>)
contact@moanadigitalhealth.com

Overview
Governments managing medicine supply at national scale face a consistent set of failures that repeat across health systems in low and middle income countries. Facilities do not know what stock other facilities have. Provinces cannot see the stock position of the facilities under their authority. The national procurement team makes ordering decisions based on historical forecasts that bear little relationship to current consumption rates. Stock-outs at facility level are discovered when medicines run out, not before. Expired medicines accumulate undetected until they are disposed of in bulk. Consumption data that should drive procurement decisions is captured on paper registers that are never aggregated.
The Moana Medical Supply System was built to address each of these failures with a three-tier digital platform that gives every stakeholder in the supply chain the visibility and workflow tools appropriate to their role. Facility pharmacists manage daily stock, dispensing, and reorder alerts. Provincial health authority officers see the stock position of every facility in their province and manage inter-facility transfers and redistribution. National procurement officers see the live supply position across the entire facility network, with consumption rate analytics and stock depletion forecasting that convert historical dispensing records into forward-looking procurement intelligence.
The system operates as both a standalone national supply chain product and as an integrated component of the broader Moana platform. Governments that have an existing Moana EHR deployment can activate the supply system within the same environment, where pharmacy dispensing records from clinical workflows automatically populate the consumption analytics layer. Governments that need supply management only, without the full clinical record system, can deploy it as a standalone national system.
Deployment follows a complete-stack model: the facility, provincial, and national tiers are delivered together in a single implementation, not phased across years. The architecture is built for the connectivity realities of Pacific Island and low-resource environments: full offline-first operation at the facility tier, delta sync architecture that minimises bandwidth consumption, and no dependency on continuous internet access for daily facility operations.
The system is designed for national deployment across large facility networks, connecting to government digital health infrastructure including DHIS2, Open mSupply, OpenHIM, and Integrated Financial Management Systems for budget-to-consumption reconciliation.
Three-Tier Architecture
Facility Tier
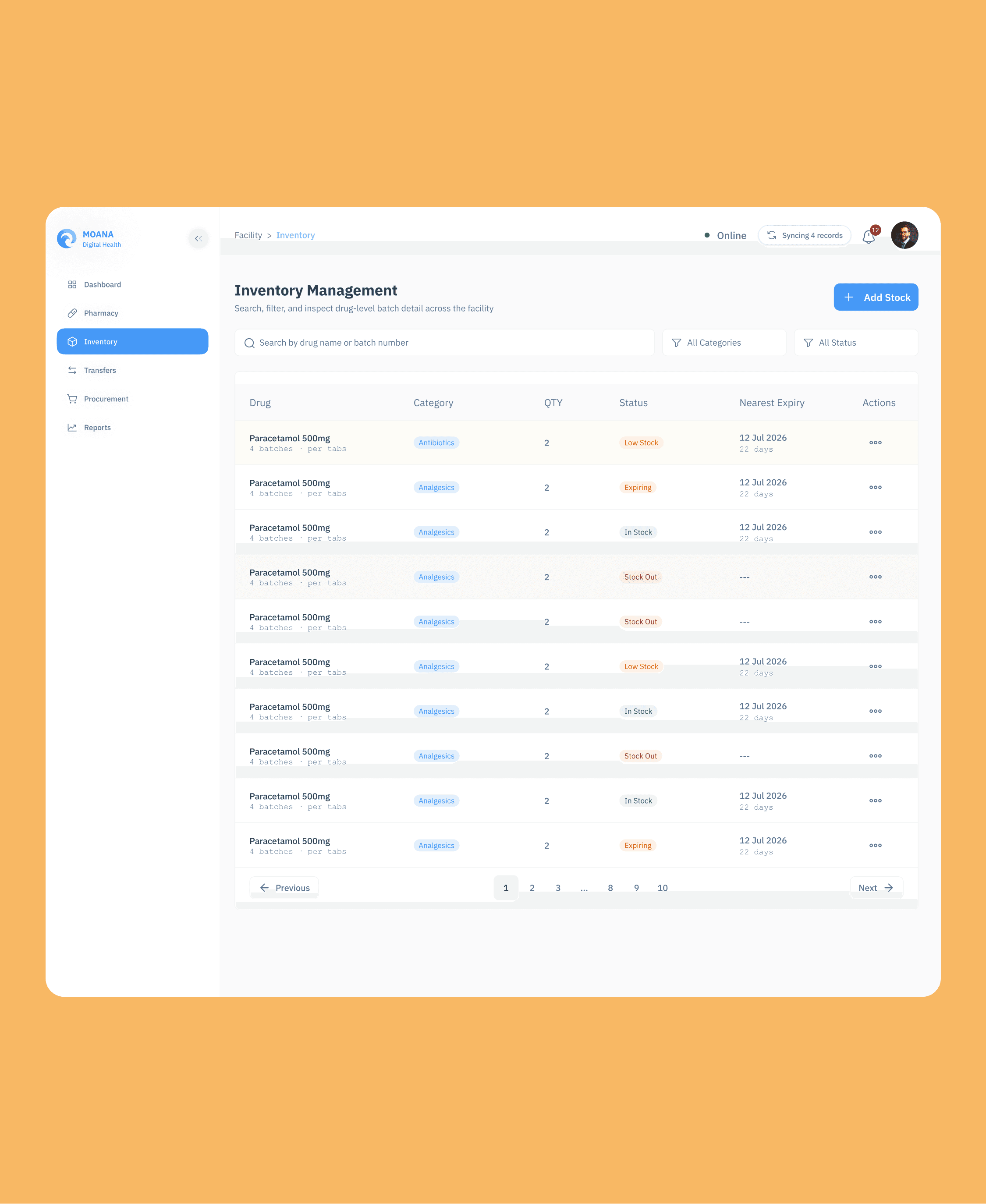
Every dispensing facility, from a rural health post to a level-five hospital, operates with a complete pharmacy inventory management stack. Stock receipt is recorded on delivery with batch number, expiry date, quantity, supplier, and purchase order reference. Dispensing creates a consumption record linked to the patient record and prescribing encounter where the Moana EHR is deployed, or as a standalone dispensing event where only the supply system is in use. Inter-facility transfer requests are initiated at the facility tier for stock redistribution within the province. Wastage and disposal events are recorded with reason codes. Reorder alerts notify pharmacy managers when stock on hand falls below defined reorder thresholds. The entire facility tier operates fully offline, with all transactions queued locally and synchronised when connectivity is restored.
Provincial Tier
Provincial health authority officers have a live stock view across all facilities within their geographic authority, without requiring access to clinical patient data. Inter-facility transfer approvals are managed at this tier: a facility requests a stock transfer, the provincial officer reviews available stock across the province, approves or modifies the request, and initiates the transfer. Redistribution planning uses the provincial stock view to identify facilities with excess stock and facilities at risk of stock-out, supporting proactive redistribution before shortages develop. Provincial supply reports are generated from this tier for provincial health authority governance and for submission to national level.
National Tier
The national dashboard provides live visibility across the entire supply network simultaneously. Consumption trend analysis by medicine, by facility, and by province is available in real time. Stock depletion forecasting projects days-to-stockout for every monitored medicine at facility, provincial, and national level from consumption history. Procurement planning tools use forecasting data to generate reorder quantity recommendations. The supplier and tender ledger manages supplier records, contract details, and pricing. Budget-to-consumption reconciliation connects procurement expenditure from the government IFMS with actual consumption records from the dispensing layer, closing the accountability gap between what was procured and what was actually used.
Core Capabilities
Real-Time Stock Visibility Across the Network
Every medicine at every facility is tracked with drug name using both proprietary and international non-proprietary names, batch number, expiry date, quantity on hand, supplier, unit cost, and reorder level. Stock status is visible in real time to facility managers, provincial administrators, and national supply officers according to their role and geographic scope. A national supply officer sees the aggregate network position for each medicine. A provincial officer sees the provincial total and facility breakdown. A facility pharmacist sees their own facility's stock only. No facility sees another facility's operational data directly.
Batch Tracking, Expiry Management, and Dispensing Order Compliance
Batch numbers and expiry dates are recorded at receipt and tracked through every subsequent movement. Automated expiry alerts at 90, 30, and 7 days before expiry give pharmacy managers sufficient advance notice to take action before medicines become unusable. First-In-First-Out and First-Expiry-First-Out dispensing compliance is enforced by the system, preventing the accumulation of near-expiry stock while newer stock is dispensed. Wastage and disposal events are recorded with reason codes: expiry, contamination, damage, cold chain breach, or other. The complete batch history for any medicine in the system provides full traceability from receipt to final disposition.
Procurement and Multi-Level Approval Workflow
Purchase request workflows move from facility through district or provincial approval to national procurement processing in a structured, tracked sequence. A facility pharmacist identifies a stock need and submits a purchase request. A district officer reviews and approves or adjusts. A provincial health authority consolidates requests from multiple facilities and approves at province level. The national Department of Health procurement team processes approved requests, raises supplier orders, and links procurement records to government financial system references. Every step is timestamped, attributed to a named user, and visible to all levels above it in the hierarchy. Rejections require a documented reason. The complete approval history is retained permanently for audit and governance review.
Consumption Rate Analytics
Consumption rate is derived directly from the dispensing pipeline rather than from self-reported facility returns. Every prescription creates a medication order. Every actual hand-out to a patient creates a dispensing record linked to a specific drug, batch, quantity, prescriber, and patient. Aggregation queries roll dispensing records into daily, weekly, and monthly consumption figures per medicine, per facility, per province, and nationally. The result is a consumption rate that is reproducible from primary dispensing records, not a self-reported estimate that facility staff must prepare separately. This is the data that drives meaningful procurement planning.
Stock Depletion Forecasting
Consumption history from the dispensing pipeline drives forward-looking stock depletion forecasts at facility, provincial, and national level. For every monitored medicine, the forecasting engine projects the expected days-to-stockout based on recent consumption rates and current stock on hand. Facilities approaching stock-out within a configurable warning window are highlighted in the provincial and national dashboards, enabling proactive procurement and redistribution decisions before shortages occur. The difference between a system that reports stock-outs after they happen and a system that forecasts them before is the difference between reactive and preventive supply chain management.
Mobility Traceability State Machine
Every leg of a medicine's journey from the central store to a patient is captured as a structured movement record. Supplier delivery arrives at the central store or area medical store as a goods-receipt movement, linked to the purchase order and supplier record. Transfer from central store to a facility creates a transfer movement that decrements the sender and, on confirmation of receipt, increments the receiver. A mobility traceability state machine tracks each shipment through SHIPPED, IN_TRANSIT, and RECEIVED states, with variance detection flagging discrepancies between the quantity shipped and the quantity received. Facility-to-patient dispensing creates the final consumption movement. Every leg is auditable from a single supply chain view.
IFMS Budget-to-Consumption Reconciliation
Integration with government Integrated Financial Management Systems connects procurement expenditure records with actual consumption data. Spend records from IFMS, covering the financial cost of medicines procured, are pulled into the supply system and reconciled against dispensing aggregates, which represent the quantity and type of medicines actually used. This reconciliation closes the accountability gap between what governments spend on medicines and what actually reaches patients, producing a budget-to-consumption view that supports both financial audit and health system performance accountability.
M&E Indicator Outputs
The system produces government-standard M&E indicator outputs aligned with national health plan frameworks and international supply chain performance standards. Direct indicators supported include access to the core set of essential medicines, the number of months per year facilities have no stock-out of greater than one week for essential medicines, medicine consumption rates by facility and province, and procurement spend per capita. All indicator outputs are generated from live system data, not periodic survey results, and are available for submission to DHIS2, donor agency reporting systems, and national health information exchange platforms.
Interoperability
DHIS2 Integration
A bidirectional DHIS2 Web API connector pushes supply aggregate indicators as DHIS2 Data Value Sets and pulls organisation unit hierarchy to ensure facility alignment with the national DHIS2 instance. Moana supply data flows into DHIS2 without requiring separate data entry at any facility. Where DHIS2 is the national health information system of record, Moana supply data enriches it rather than duplicating it.
Open mSupply Integration
Where Open mSupply is already deployed at the area medical store level, Moana connects to read and write consumption and stock data, allowing the two systems to coexist without conflict. Open mSupply retains its area medical store function. Moana provides the facility-tier and national-tier visibility that Open mSupply does not cover.
IFMS and HL7 and FHIR Connectivity
FHIR R4 is supported natively with fifteen or more resource types including Medication, MedicationRequest, MedicationDispense, and SupplyDelivery. HL7 v2 gateway connectivity supports legacy hospital systems. OpenHIM mediator registration supports national health information exchange architectures in countries following the OpenHIE specification. IFMS integration is implemented as a controlled data export for budget-to-consumption reconciliation.
Who Uses This Module
Facility Pharmacists and Dispensary Staff
Daily stock management, dispensing, receipt, and reorder alert management at the facility level.
Provincial Health Authority Officers
Provincial stock oversight, inter-facility transfer approvals, redistribution planning, and provincial supply reporting.
National Department of Health Procurement Teams
National stock visibility, consumption analytics, depletion forecasting, procurement planning, supplier ledger management, and budget-to-consumption reconciliation.
Development Partners and Donor Agencies
Access to M&E indicator outputs and supply chain performance analytics for programme reporting and accountability frameworks.
How This Connects to the Rest of Moana
Where the full Moana EHR is deployed alongside the Medical Supply System, pharmacy dispensing records from the clinical workflow automatically populate the consumption analytics layer without any additional data entry. Prescription data from Clinical Care Management feeds directly into the dispensing pipeline. Stock levels from the Medical Supply System feed expiry alerts and essential medicine monitoring in the Pharmacy module. Supply programme indicators feed the national Public Health Surveillance System for Ministry reporting. The billing module connects pharmacy dispensing costs to patient episode financial records.
Standards and Interoperability
FHIR R4 with 15 or more resource types, DHIS2 Web API, Open mSupply connector, OpenHIM mediator registration, HL7 v2 gateway, and IFMS controlled export. All data is hosted in-country or in a government-specified cloud region. No data leaves the country without explicit government authorisation. Per-service scheduled backups with documented restore tooling support data sovereignty and disaster recovery requirements.